
In Parts 1 through 6, I explained the Healthcare Incentives Framework, which is useful for clarifying the necessary ingredients of an optimal healthcare system. Those are the pre-requisite readings to understanding this post, and I will not fully summarize or provide the rationale for them here. But, just as a reminder, Parts 1 through 6 culminated in the goal of getting market share to flow to higher-value providers and insurers, which would be enabled through three critical inputs to decision makers/patients: (1) multiple options, (2) the ability to identify the highest-value option, and (3) incentives to choose the highest-value option. As barriers to those three inputs are minimized, any healthcare system will begin to evolve to deliver higher and higher value. This is the only way to unlock sustained value improvement in healthcare systems.
An important point about this framework is that it is, in a sense, welfare-spectrum neutral, meaning the principles apply to healthcare systems that sit at any point on the welfare spectrum, from libertarian-type systems to fully government-run systems.
Now let’s imagine up some concrete examples of what different types of systems might look like if we built them from scratch using the ingredients from the Healthcare Incentives Framework.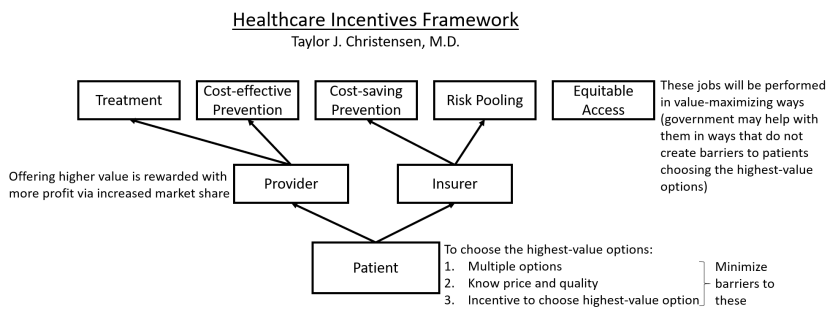
A Libertarian-type System
In this system, there are many private insurers all offering creative and innovative health insurance plans. Their efforts are focused on trying to maximize cost-saving prevention so they can lower their costs and then outprice their competitors. This has led to many ways of keeping people out of hospitals and emergency departments. But since health insurance is an inherently complex product, there are some standardized levels of coverage that have been agreed upon to help people compare those plans apples to apples. This standardization has been implemented in a way that maximally improves comparability with minimal limitation on plan design flexibility. Multiple health insurance comparison shopping websites have arisen, all highlighting those standardized coverage levels, differences between plans, and clear pricing.
An important aspect of these insurance plans is that most of them require the enrollee to pay some part of the price differential between providers; this did not need to be mandated because insurers found that they are able to price premiums more aggressively when they have implemented those cost-sharing characteristics. The plans that do not have this feature are much more expensive, but some people prefer them because they don’t ever need to worry about prices when choosing providers.
There is no requirement for people to buy health insurance, but because there is also no guarantee of care if someone without insurance has a catastrophic medical expense, many people are motivated to buy catastrophic coverage. The rest of their care they buy a la carte out of pocket.
Many of the poor, as well as people with chronic expensive medical conditions, are priced out of the insurance market, but private charities have cropped up that assist with this for most of them.
Looking at the provider side, nonprofits have played a leading role in establishing standards in provider quality metric tracking and reporting. These nonprofits also certify the quality information being reported by providers, so patients are able to compare the quality of different providers apples to apples. The quality metrics being reported and certified are determined by what patients find most relevant in helping them decide between providers for each service they are shopping for. Similar to the health insurance shopping websites, there are provider shopping websites presenting those standardized metrics alongside providers’ advertised prices.
Because providers are assured increased market share when their value goes up relative to competitors, there is a great variety of innovation toward crafting high-value care experiences for patients. Most of the value improvements are in the form of cost-lowering innovations because of the downward pressure on price exerted by the uninsured population and the price-sensitive insured population. Providers have particularly found that shifting the location of care to less expensive settings (including even the patient’s own home) and shifting to relying more on narrowly trained provider types (particularly for treatments that are relatively algorithmic) is very effective at lowering costs. Suppliers of healthcare devices have also found that they are more successful as they focus on developing lower-cost devices, even if that means sacrificing some amount of quality or features. And since government regulations have been kept to a minimum, all these innovations have been allowed to progress and flourish quickly. This occasionally results in unsafe practices and devices cropping up, and individuals have been hurt in the process, but people have felt that the rapidity of innovation that has improved so many lives has been worth that cost. And any practice that proves to be unsafe is exposed quickly in this marketplace.
Providers have also found that, when patients are shopping for a provider, they are looking for a specific well-defined service or bundle of services, such as a year’s worth of chronic disease management, a CT scan, a hip replacement (including all the pre-op workup and the post-op rehab), or a diagnostic evaluation. This has led to standardized bundles of services (also certified by those non-profits), which has made shopping for healthcare services easier and also enhanced the ability to compare the prices from one provider to another.
This system is not perfect. Some people choose not to buy insurance and then have to declare bankruptcy when they have an expensive care episode (or end up not getting care due to inability to pay), and some people want to buy insurance but are frustrated that they cannot afford it, although this number is decreasing each year. Providers face challenges dealing with multiple insurance plans with different reimbursement schemes and coverage rules. And unsafe practices or innovations crop up every so often that harm patients. But, overall, the value delivered by insurers and providers increases rapidly as insurers find new ways to prevent care episodes, and, for the care episodes that cannot be prevented, providers find ways to make care safer, more convenient, and more affordable.
A Single-payer System
With the government running the single insurance company for this system, they have been able to easily implement many of the needed aspects of an optimal healthcare system. They automatically cover all known cost-saving and cost-effective preventive services without copays, which includes population-based preventive services but also focuses more and more on targeting extra services to high-utilizing patients to prevent hospitalizations and ED visits. Their cradle-to-grave time horizon has helped this immensely.
The prices the insurer assigns to services are not firm but are rather considered to be the “maximum allowable reimbursement,” so any provider that wants to charge a lower price will have the freedom to do that. And providers who innovate and find ways to charge less win market share because the insurance plan’s cost-sharing policies require people to pay less out of pocket when selecting a less expensive provider. The insurer has also found that paying a single fee for standardized bundles of services has motivated a great deal of provider innovation and cooperation.
Together, all these reimbursement policies help to prevent as many care episodes as possible and minimize the cost of the episodes that are not preventable.
The insurer’s fee schedule also includes a multiplier to adjust for regional cost variations, and they leverage this to increase reimbursement in underserved areas as well, which has especially helped rural areas maintain enough providers.
As a condition of being accepted as in-network by the insurance plan, providers are required to use an electronic medical record that is able to decode and record to the patient’s secure cloud-based personal health record. Providers are also required to report specific quality metrics. These quality metrics are never used for giving bonuses, but they instead focus on the aspects of quality that patients find most relevant when they’re trying to decide between provider options. The insurer operates a single website that lists all in-network providers along with these risk-adjusted quality metrics and each provider’s prices (displayed as the amount the patient will be expected to pay out of pocket).
Providers appreciate this system for many reasons. They only deal with a single insurer, which minimizes insurance-related overhead expenses and gives them a single set of incentives to respond to. They are completely free to build hospitals and clinics wherever they think they will be most profitable. And they can organize care however they want provided they adhere to the safety and reporting regulations.
Now, having seen the main aspects of this system, let us consider the impact of not adhering to the Healthcare Incentives Framework’s requirement of having multiple insurer options. Recall that the jobs insurers are primarily responsible for are risk pooling and cost-saving prevention. And the reason having multiple options is desirable is because—assuming patients can identify and then choose the highest-value insurance plans—insurers will have a profit motive driving them to innovate to find ways to increase the value they deliver, which especially means finding ways to do more cost-saving prevention that will result in more care episodes being prevented, thus lowering the total cost of care and insurance prices. With a single government-run insurer, that innovation and its attendant benefits will be curtailed. Clearly there are many compensatory benefits, including simplicity, reduced administrative overhead, uniform incentives, and a straightforward way of achieving a society’s goal of universal access to insurance. Depending on the priorities of the country, these benefits may outweigh the costs. It is a question of values. But the decision becomes clearer when the costs and benefits of each option are understood.
A Government-run System
This system, like the single-payer system described above, has a single insurer that is run by the government. But here the government also owns all the healthcare facilities and employs all the healthcare providers.
On the insurance side, reimbursement policies are familiar, with “maximum allowable reimbursements,” bundled pricing, differential cost-sharing for patients, and a website reporting the quality metrics and prices (out-of-pocket costs) of providers. The insurer also has a robust department working on preventing care episodes by finding innovative ways to keep people healthy.
But what about the provider side? Initially it may seem that patients only have a single healthcare provider option, but just because a single entity owns all the hospitals and clinics does not mean they are all the same. In this system, the government determines where healthcare facilities will be built and what services they will provide, but it allows great freedom in their operation. At every facility, providers are able to organize care however they like, and they are also free to charge any price as long as it is at or below the maximum allowable reimbursement for each service. They have great motivation to put in the effort required to find ways to lower costs (thereby enabling them to charge lower prices) and improve quality because they receive bonuses that are calculated based on the amount of money they saved the system (the number of patients treated multiplied by how much less than the maximum allowable reimbursement each of those patients was charged).
Because the insurer and providers are all operating under one roof, the billing in this system is particularly simple. Some specific requirements are in place for the purpose of accumulating data that will help track for problems in the healthcare system, but there are no complex billing codes or arcane documentation requirements. When providers document a patient encounter, they do so for the purpose of communicating to other providers what they thought and did.
Government healthcare expenditures in this system are sustainable mostly because providers are actively innovating to improve value—much of which results in them being able to lower prices so they can earn bonuses.
Overall, this system has been organized in a way that, despite the government ownership of providers, maintains the ability to reward value with market share, which drives value improvement. The insurance side also innovates to prevent care episodes by leveraging its cradle-to-grave time horizons and connections with other non-healthcare public health sectors.
There are barriers to provider innovation compared to other systems. Providers face the upside of potential bonuses for doing well, but there is not necessarily much downside risk in providers who are mediocre or worse and still getting paid their stable salary. In any other market, the risk of being forced out of business due to lost market share drives competitors to innovate to improve their value so they can become profitable, but in this system the worst-case scenario is that the government closes their clinic and relocates those providers elsewhere. Additionally, many innovations require new types of facilities or caregivers, or they require cooperation between multiple types of providers, which can be difficult when providers have limited control over facility design, placement, and reimbursement contracts.
The effects of these innovation barriers are difficult to quantify, but they need to be balanced with the benefits of a reduced documentation burden, a simpler billing system, and a more reliable dispersion of healthcare services across the country.
Conclusion
Policy makers overseeing any type of system need to understand their system’s current barriers to the three critical inputs: multiple options, ability to identify the highest-value option, and incentive to choose the highest-value option. (Many of the most common barriers to those three inputs are outlined in Part 6.) They need to understand that those barriers are the primary inhibitors of their healthcare system evolving to deliver increasingly higher value for patients over time. And as they enact policies that eliminate those barriers, they will see a predictable chain reaction of more patients choosing higher-value insurance plans and providers, those higher-value competitors earning more profit, and parties in the healthcare system beginning to innovate to deliver higher value, all of which will result in the healthcare system transformation that is sorely needed the world over. Policy makers who understand this Healthcare Incentives Framework are also empowered to propose and support policies that expand access in ways that do not create new barriers to those three critical inputs.
As healthcare reforms begin to take this focused direction, the innovations and value improvements will be exciting to watch!
In Part 8, I will conclude this series by imagining how the U.S. healthcare system might look with the Healthcare Incentives Framework fully implemented.

9 thoughts on “Building a Healthcare System from Scratch, Part 7: Concrete Descriptions of Some Optimal Systems”