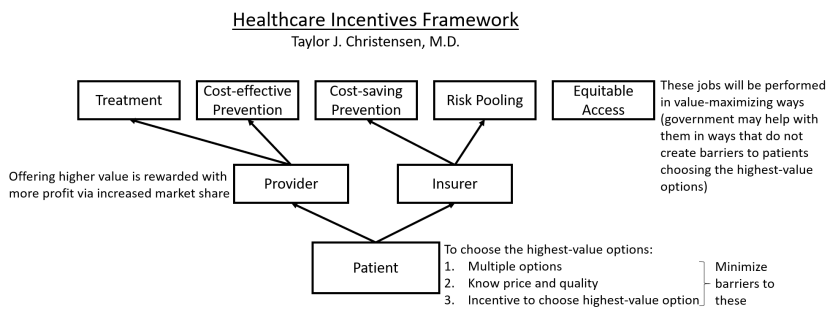
In Part 5, we talked about the three requirements for getting market share to flow to the highest-value options, which is necessary if we want higher-value parties (insurers and providers) to be rewarded with profit. The context for why this is the crucial feature of our optimal from-scratch healthcare system is discussed in parts 1, 2, 3, and 4.
As a reminder, those three requirements were for patients to have (1) multiple options, (2) the ability to identify the highest-value option, and (3) incentives to choose the highest-value option. Let’s look at examples of the common barriers to each of them so we will know what to avoid when we build our optimal healthcare system.
Multiple Options
Our goal: Avoid any policies that directly or indirectly limit the number of competitors in a market.
For providers, this means allowing them to build hospitals and clinics whenever and wherever they want. They will not do this with reckless abandon because they will know that, if they choose to build in a new region and end up delivering lower value than the incumbents, they will not get many patients and their new endeavor will not be profitable.
For insurers, this means avoiding regulations that make it difficult for them to enter new markets. Nationally standardized regulations will simplify the process of selling insurance in multiple markets, but this does nothing to ease insurers’ greatest challenge of entering new markets, which is the challenge of negotiating prices with providers in that region. But having many provider options in a region should help with this.
And as for things that affect both providers and insurers, we will need good antitrust laws to prevent too much consolidation. And we will need to avoid policies that limit the freedom of them to vary their price and quality so that they can offer unique value propositions (otherwise we end up with many options that all are effectively the same, which defeats the purpose).
Identifying the Highest-value Option
The barriers to this are different for providers and insurers.
On the insurer side, the most difficult aspect of identifying the highest-value option is being able to predict which mixture of premium, copay, deductible, coinsurance, etc. will cover what you need in the cheapest way possible, as well as identifying/predicting which services will be needed and whether they are covered in the benefits. Having some standardization can make this much simpler (but still challenging), such as what healthcare.gov does with multiple standardized quality tiers of insurance plans and grouping all those options together to be compared apples to apples.
On the provider side, one of the first challenges is getting people to recognize that they have multiple options that are of very different value. In almost every other industry, people are great value shoppers, but they have been conditioned historically not to even think about it when choosing healthcare providers, which is probably a consequence of the chronic unawareness of the huge variations in the quality of providers as well as the third-party payer system that so often causes people to pay the same no matter which provider they choose. This is one reason why healthcare provider quality reporting websites are so infrequently used even when they are available.
The other issues with identifying the highest-value providers can be divided into barriers to knowing price beforehand and barriers to knowing quality.
Barriers to knowing price beforehand: The biggest one is uncertainty about what services will be needed—for example, most people do not present to the emergency department with a diagnosis already, nor can they predict what additional complications might arise during a hospitalization. But for specific, well-defined episodes of care, such as an elective surgery, there are great ways to make prices knowable beforehand (look up bundled pricing for an example).
Barriers to knowing quality: People do not know where to find quality information even if they do go looking for it. And if they find it, most of what they find are quality metrics geared specifically toward comparing providers for the purpose of allocating bonuses rather than quality metrics that actually provide metrics that are relevant to helping a patient choose between providers. For example, a hospital’s overall mortality rate or readmission rate has little bearing on the quality of care a patient will receive for something like a straightforward elective gallbladder removal. Standardized, easy-to-understand, appropriately risk-adjusted, patient decision-oriented quality data are needed.
And the last thing to mention in this section are the barriers to identifying the highest-value option that will not likely be overcome. For example, medical emergencies don’t allow time to make a thoughtful decision about which hospital to go to. And low health literacy is a barrier for many people. And there are many important aspects of care that cannot easily be measured, such as a primary care doctor’s ability to diagnose the cause of ambiguous symptoms. Does the presence of these more insurmountable barriers mean that no health system will ever be able to get market share to flow to the higher-value options? No—even if many decisions about which provider to go to are not particularly logical or value-focused, as more people start choosing providers based on price and quality information, higher-value providers will begin to win more market share and the desired incentive scheme that motivates value-maximizing behaviors will arise.
Incentives to Choose the Highest-value Option
Even when people (1) have multiple insurer and provider options and (2) are able to identify the highest-value options, there are still barriers to them choosing the highest-value options.
The first barrier is when anyone but the patient is acting as the decision maker. These alternative decision makers typically have a financial stake in the decision and want to choose the cheapest option without regard for quality. For example, insurers that offer very narrow networks act almost like a first-cut decision maker to narrow patients’ possible provider choices down to only providers that are willing to accept the lowest prices. Patients/patient advocates should be the decision makers because only they will adequately weigh the quality aspects that are most important to and impactful on them.
But even when the patient is the decision maker, they will ignore prices if they are required to pay the same amount regardless of the provider or insurer they choose. This is usually not an issue with insurance plan selection, but it is a major issue with provider selection. For example, flat copays require the same payment from the patient regardless of the full price of the providers. High-deductible plans solve this problem for any service below the deductible, but, once that deductible is surpassed, they have the same problem. Ideas such as reference pricing, multi-tier provider networks, or even paying patients for choosing lower-cost providers can help with this.
Summary
If the above discussed barriers to the three requirements for getting market share to flow to the highest-value options are minimized, the healthcare system will naturally and continuously evolve toward higher value because it will motivate providers and insurers to perform their jobs in value-maximizing ways. Government interventions may still be considered for areas where natural incentives will not motivate those parties to do all the jobs we want them to do (particularly in the area of equitable access), but the “healthcare market” will start functioning to benefit patients and what they value.
This concludes the big-picture explanation of this Healthcare Incentives Framework. In other words, we have now discussed all the ingredients that need to go into an optimal from-scratch healthcare system. In Part 7, we will solidify the implications of this framework by imagining up a few examples of different types of healthcare systems with the Healthcare Incentives Framework implemented to show how all those ingredients can come together.