I work as an inpatient internal medicine physician, usually referred to as a hospitalist. People sometimes hear about how complex billing and coding are in our system, so today I’d like to give a taste of my experience with this.
Before I explain this, I should be clear that any provider’s goal with billing is to bill honestly to the highest amount they can for the necessary work they’ve done. Not billing for something that we are legally allowed to bill for is leaving money on the table and unnecessarily lowers our income. So keep in mind that, when I talk about billing the maximum possible, this is an honest and appropriate goal that is very different than taking advantage of the system or committing some kind of fraud.
Each day when I see a patient, I am expected to write a daily progress note. Originally, these were strictly for communication with other caregivers so everyone would know what’s going on with the patient and nurses would know what needed to happen for patients. Then EMRs came along, the primary motivation behind them being that it would streamline the process of sending bill to insurers. Helping with the clinical care of patients was a secondary purpose. I’m not sure whether the data-capturing ability of EMRs allowed coding policies to become more detailed/specific/complex, but it sure seems that way, as you will see.
When a patient is in the hospital, the hospital charges a bill and each doctor who sees the patient charges a bill. This week, I’ll focus on the hospital side.
Hospital contracts with insurers are mostly based on DRGs, which stands for “diagnosis-related groups.” Essentially, the hospital sends to the insurer a list of the diagnoses that were treated during the hospitalization, and then, based on that list, the patient is assigned to a certain DRG, and the hospital gets paid the standard amount for that DRG. There are a bunch of little adjustments here and there for location, hospital type, etc., but that’s the essence of it.
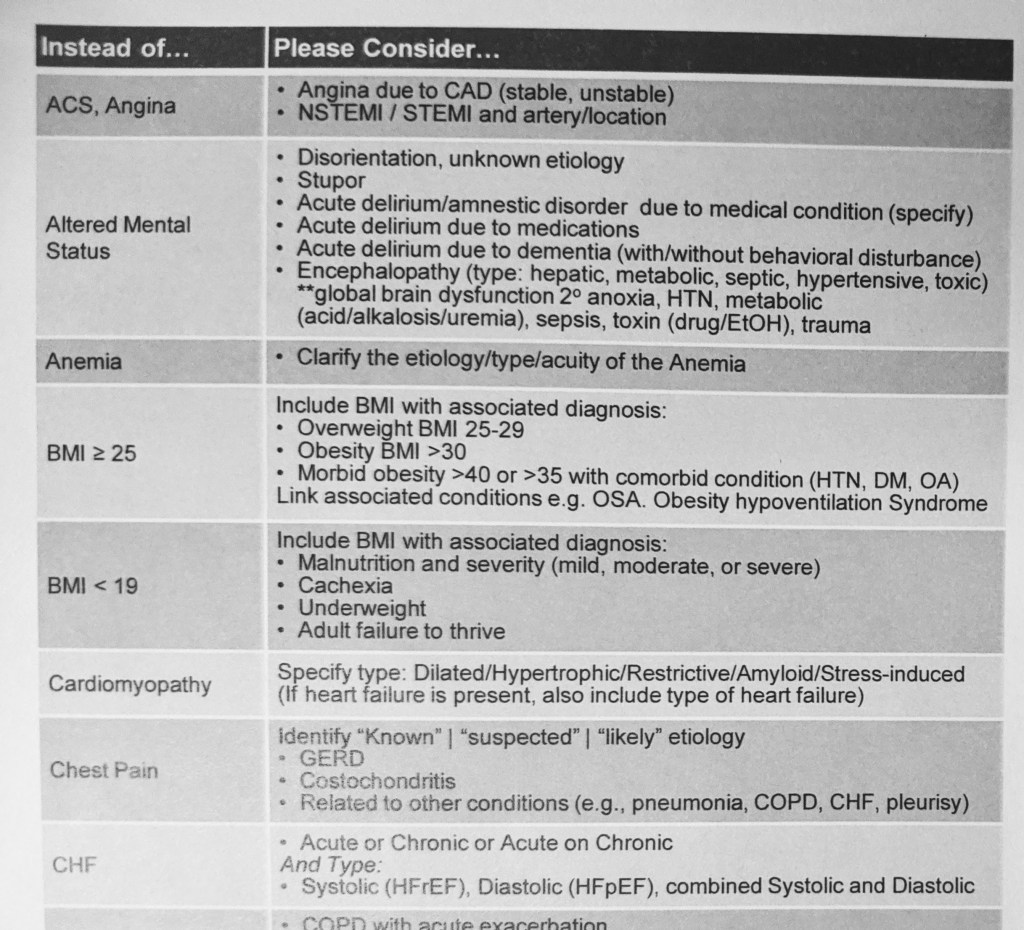
As a hospitalist, I am usually the primary doctor over a patient’s hospitalization, so making sure all the right diagnoses are listed in the patient’s chart is super important if I want the hospital to get paid for the work we did. It would be nice if there were just a few different DRGs, but there aren’t. There are 1,000 arcane rules that make a big difference in which DRG the patient ends up getting assigned to, which means trainings about how to add the right DRGs take up a significant percentage of hospitalist meetings (as opposed to trainings on how to be better doctors!). They give us pamphlets full of suggestions on how to correctly add problems to the patient’s problem list. Here’s part of a single page of one of these multi-page pamphlets:
When I am working in the EMR, we also have some built-in software through which coders somewhere who are reviewing every single patient’s chart will send me messages (“coding queries”) with suggestions about which additional problems to add or how to make diagnoses more specific to get the patient lumped into a higher-paying DRG. It’s implemented very well, but it definitely disrupts my workflow.
Another issue is that sometimes these DRGs use old diagnostic rules. For example, anytime someone has at least two of the following–high heart rate, fever, high white blood cell count, high respiratory rate–there is a sepsis alert that tries to get me to add that to the problem list (and make sure you specify what the source is, which organ system is involved, and how severe it is!). The problem is, that’s the old definition of sepsis that has been proven to be less useful than newer definitions. So sometimes my clinical judgment says a patient doesn’t have sepsis, but I have to remember the old definition to make sure I add it to the problem list where that definition fits.
And don’t worry–if I forget to add something and the patient gets discharged, those coders can always track me down and have me sign forms that go into the patient’s chart stating there were other problems that were not added but that we took care of in the hospital.
All of this results in many patients having problem lists in excess of 30 items. It’s completely overwhelming! These lists are automatically inserted into every note I write and form the template for writing my problem-based assessment and plan, which means my assessment and plan looks incredibly long and interferes with communicating to other caregivers what’s important and what’s actually going on with the patient.
Not only is the list burdensome because of its length, but also the names of these problems are often less useful. If I wanted to, I could take the time to go and manually change them in the patient’s chart before generating my daily progress note, but then it’s that much extra administrative time I’m taking. And, if I manually change the problem name, now the name is different than the underlying problem code’s name, which may mean I or a colleague who takes over the patient’s care will not notice if the problem code becomes inaccurate or not specific enough, causing further confusion and messages from coders.
Oh, also this all supposes that the patient is sick enough to be considered an “inpatient” when they are here. If they aren’t sick enough (based on a whole different set of criteria), then they are only here under “observation,” and DRGs don’t apply, so the patient is billed for each individual service done.
So, that’s just a taste of the hospital side of billing. Next week, I’ll give you a taste of how provider billing works.

