I got an email this week from my hospital system introducing the team of administrators who are managing the CME (continuing medical education) credit card they give to providers. You see, providers are given an annual stipend that they can only use for CME activities, such as trips to medical conferences, and this is the card we are supposed to use for those expenses. I read the email and looked around to see if anyone else thought it was ludicrous that there is a whole “team” of people dedicated to something like this.
The issue of unnecessarily high administrative expenses in the U.S. healthcare system has been on my mind ever since the recent article in JAMA detailed the “6 waste domains” in our healthcare system and pegged administrative expenses as the biggest one. So, today, I’m going to explain how I calculate administrative expenses in our healthcare system. I believe it’s more intuitive than other approaches because it follows the flow of money through the healthcare system and shows each point where some of the money is siphoned off for administrative expenses. Disclaimer: I’m using nicely rounded numbers and lots of assumptions for the sake of clarity.
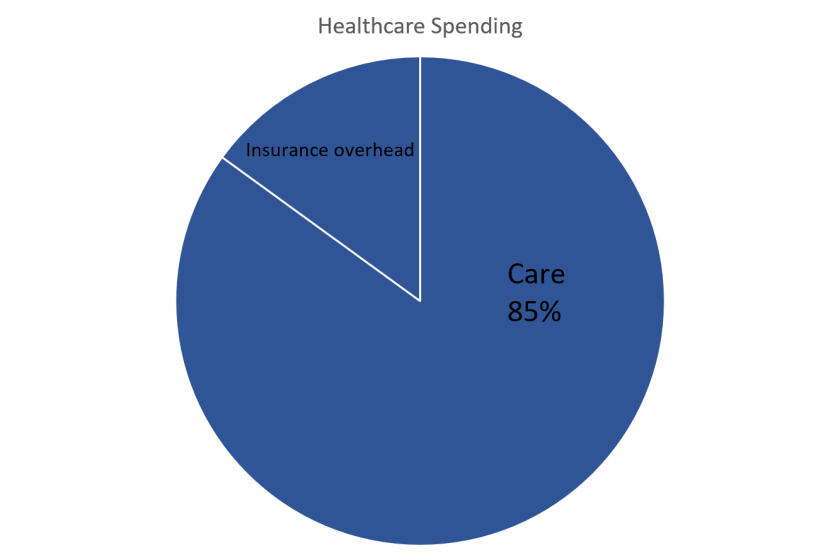
Money enters our healthcare system when the patient pays insurance premiums. Let’s say the amount of each dollar paid to an insurer that gets spent on actual care is around 85 cents (their “medical loss”), which means 15 cents goes to administrative expenses in the form of insurance overhead:
And then what about the 85 cents that is being paid to healthcare providers? Studies have used reports submitted to Medicare to estimate the percent of hospital revenue that goes to administrative expenses, and they come up with about 25% in the 1990s, but it has been rising. So if we guess that about 29% of those 85 cents paid to hospitals and other facilities goes to administrative expenses (like teams of people managing CME credit cards, plus armies of coders, “revenue cycle managers,” and so many more), that works out to be 25 cents in additional administrative expenses:
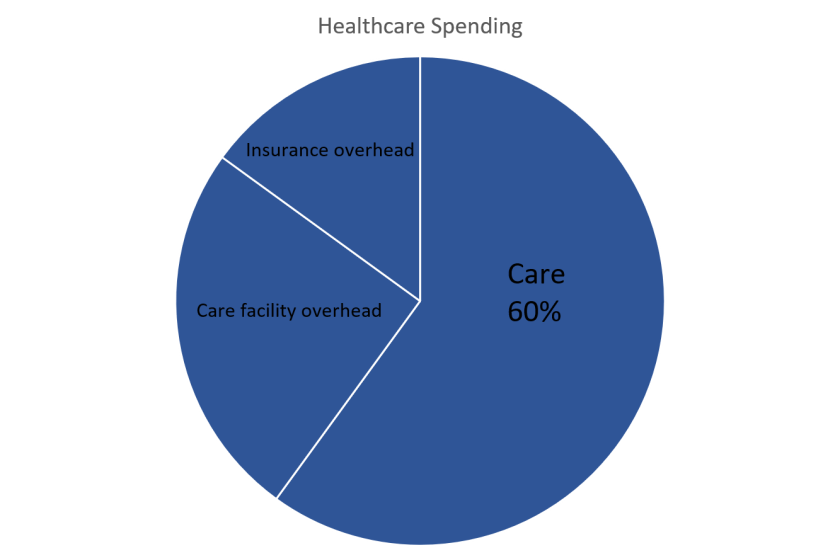
Of the 60 cents left, it’s going to actual care, such as paying caregivers and buying other care-related things like drugs and devices, right? Not so fast. First off, let’s assume about half of that 60 cents goes to drugs and devices (both of which are generally overpriced, but that’s a different subject I’ve written about before). This leaves 30 cents of every healthcare dollar for caregivers. And if 100% of caregivers’ time were devoted to care, we would be dancing and singing every day we go to work. Instead, we spend a great portion of our time on “the system,” dealing with insurance issues, federally mandated trainings, documentation time ensuring billing and diagnostic codes are accurate and thorough, etc. etc. etc. When accounting for all of those factors, it adds up to much more than the estimated 15% of my time dedicated to administrative tasks. I’d peg it closer to 30%. Others would probably say 50%. Things seem to be worse here in the U.S. compared to in the motherland. Anyway, that means roughly 15 cents of every dollar can be attributed to caregiver overhead:

I will not include in here the additional money providers have to be paid to compensate for the high cost of medical training and malpractice insurance. So, overall, I’m guessing that 50 cents of every dollar that enters the healthcare system goes to non-care things, which we call administrative expenses. Now, this number is very different from the number researchers came up with in the study cited above, which estimated that the overall administrative cost was around 30%, but they’re adding things up differently. That’s fine. We’re counting differently. But the important thing is looking at each of those siphoning points and understanding why they have higher-than-necessary admin costs. I won’t go into detail on that today, but I believe the main factor is the complexity of the system. So. Much. Complexity. We need a simpler healthcare system. I have described a few options here and here. The simplicity we could achieve may come partly by direct efforts to simplify, but I believe it will be more a side-benefit of making the other changes that are necessary in our system.

Isn’t that the real advantage of direct primary care and why it could be a solution to the mess we have now? I have had DPC docs come on and talk about their practices at HFMA events. Take aways
1) The use exercise studio software to collect the monthly fees. No insurance billings
2) No reporting, only real paperwork is maintaining notes and issuing scripts/orders for tests
3) Most provide pretty much unlimited access. A lot use phones, video chat to provide interaction.
4) They control their processes. They love not being dictated to on how to do things.
Most of these docs have been able to enter into numerous contracts for maintenance drugs and various lab and imaging. One mentioned a CMP for $16 and a MRI for $400, less that one third of the “traditional” cost. There’s your overhead! A lab manager at one of the events claimed she paid more than the $16 for the reagents to do a CMP and that it didn’t make sense. More overhead. I would be wondering why am I spending so much and my costs so high in comparison.
In LEAN terms, DPC is the ultimate elimination of waste. The provider contracts with the patient to provide a scope of services the patient wants. No one in between. In free market terms, good providers will be sought out by reputation. Natural incentives exist to provide good care and reduced need for visits. One can build their patient base to the size that fits their work habits and lifestyle.
Some insurance plans have already recognized this concept and are carving out primary care to providers/groups using this model. Event state Medicaid plans are testing. How much value is there in $60 or $80 per month to be able to see a provider as much as needed and get most of the routine labs and tests for peanuts? Compare that to the high deductible on today’s insurance options.
Yes, thanks for sharing! That is a perfect example of delivering care with a simpler structure, and it illustrates my point very well. Lower overhead in all three categories I wrote about.
One other point about DPCs: The potentially negative incentive DPC practices have is to avoid care, but that is minimized when quality information is available. If even just something as simple as patient satisfaction scores could be available to patients considering joining a DPC clinic, the clinics that keep people happy will get more in demand, then they are rewarded with more profit (either by leveraging their popularity with higher prices or by taking on more patients).