We established in prior parts of this series that, in this Healthcare Incentives Framework, there are specific identifiable jobs we want a healthcare system to do for us, and that there are parties that have incentives to perform those jobs for us. The focus then turned to how to get those parties to perform those jobs in ways that maximize value, which we saw is achieved by rewarding them with more profit when they perform their jobs in higher-value ways. And in Part 4, we saw that the only effective way to do that is by getting market share to flow to the higher-value options. In this post, we examine what needs to happen for people to choose those higher-value options.
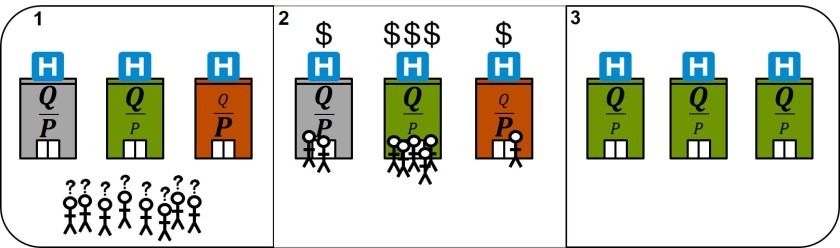
There are three requirements that all must be in place at the same time to enable someone to choose the highest-value option:
Requirement 1: Multiple options. This one seems straightforward–no market share can flow anywhere if there is only one option available. But there is another, less obvious aspect of this. Parties also need the freedom to vary their price and quality in ways that create unique value propositions, otherwise they will all look pretty similar, so the effective options people have would be severely limited, even if the total number of options is not. For example, if there is a price floor created by some administrative pricing mechanism, it will prevent any innovation that lowers quality a little bit but significantly lowers price. Why? Because those parties contemplating that kind of innovation will know that, without the ability to offer prices significantly lower than their competitors, they will be unable to win the market share necessary to make their innovation profitable.
Requirement 2: Ability to identify the highest-value option. Remember that value is determined by two things: quality and price. People choosing from among multiple providers or insurers need to be able to compare, apples to apples, the quality and price of all their options before they select one. But having apples-to-apples comparable price and quality information is not enough. The quality information would have to be simple enough to be easily understood and also relevant to the specific dimensions of quality people actually care about. And price information would need to reflect the expected total price of the product or service, otherwise it’s mostly useless. Both quality and price can be challenging in healthcare, which creates barriers to people being able to identify the highest-value option, but those barriers will be discussed in part 6 of this series.
Requirement 3: Incentive to choose the highest-value option. Even if people have multiple options and are able to easily tell which is the highest-value option, they will not choose that highest-value option without the right incentives. This applies to both their insurance plan selection and their care providers selection. Consider this example about choosing the highest-value care provider: suppose a patient has the choice to have a procedure at a nearby world-renowned hospital (95% success rate, $80,000) or the local community hospital (92% success rate, $40,000). Further suppose that this patient will pay $10,000 out of pocket (their annual out-of-pocket max) regardless of which hospital they choose. Which will they choose? An additional 3% chance of success for an extra $40,000 seems steep, but since they’re not paying the difference, most people would go for the world-renowned hospital regardless of the difference. Extracting the principle from this example, people need to pay more when they choose a higher-priced provider (or less when they choose a lower-priced provider); this doesn’t necessarily mean they always need to pay the complete difference between the two, but they at least need to pay some of that difference. Same goes for the quality aspect of value. If someone other than the patient (say, the insurance company) is choosing where the patient will receive care, they generally care a lot more about the price than about the quality differences between the options since they aren’t the one who bears the consequences of going to a lower-quality option. So, in summary, regardless of whether the discussion is about choosing providers or choosing insurance plans, the individual making purchase decisions needs to bear the price and quality consequences of the decision.
By now it should be clear that if any of these three criteria are not fulfilled, market share will not flow to the highest-value options, and the whole incentive scheme we are creating falls apart.
There are, you may have figured, many many barriers to these things working in current healthcare systems, some of which would be present even in our optimal healthcare system we are building. But that’s the topic of Part 6.

 In parts
In parts